From Surf Wiki (app.surf) — the open knowledge base
Vasculitis
Medical disorders that destroy blood vessels by inflammation
Medical disorders that destroy blood vessels by inflammation
| Field | Value |
|---|---|
| name | Vasculitis |
| synonyms | Vasculitides |
| image | HSP_Vasculitis.jpg |
| caption | Petechia and purpura on the lower limb due to infection-associated vasculitis. |
| field | Rheumatology, Immunology |
| pronounce | |
| symptoms | Weight loss, fever, myalgia, purpura, abdominal pain |
| complications | Gangrene, Myocardial infarction |
Vasculitis is a group of disorders that destroy blood vessels by inflammation. Both arteries and veins are affected. Lymphangitis (inflammation of lymphatic vessels) is sometimes considered a type of vasculitis. Vasculitis is primarily caused by leukocyte migration and resultant damage. Although both occur in vasculitides, inflammation of veins (phlebitis) or arteries (arteritis) on their own are separate entities.
Signs and symptoms
The clinical presentation of the various vasculitides on the skin and internal organs is mostly determined by the diameter or size of the vessels mainly affected. Non-specific symptoms are common and include fever, headache, fatigue, myalgia, weight loss, and arthralgia.
All forms of vasculitides, even large vessel vasculitides, may cause skin manifestations. The most common skin manifestations include purpura, nodules, livedo reticularis, skin ulcers, and purpuric urticaria.
| Type | Name | Main symptoms | Primary large vessel vasculitis | Primary medium vessel vasculitis | Primary small vessel antineutrophil cytoplasmic antibody (ANCA)–associated vasculitis | Primary immune complex small vessel vasculitis | Primary variable vessel vasculitis | Single-organ vasculitis | Secondary vasculitis | |||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Takayasu arteritis | last1=Johnston | first1=S L | last2=Lock | first2=R J | last3=Gompels | first3=M M | title=Takayasu arteritis: a review | journal=Journal of Clinical Pathology | publisher=BMJ Publishing Group | volume=55 | issue=7 | date=2024-03-14 | pages=481–486 | pmid=12101189 | doi=10.1136/jcp.55.7.481 | pmc=1769710 }} | ||||||||||||||||||||
| Giant cell arteritis | last=Hoffman | first=Gary S. | title=Giant Cell Arteritis | journal=Annals of Internal Medicine | volume=165 | issue=9 | date=2016-11-01 | pages=ITC65–ITC80 | issn=0003-4819 | doi=10.7326/AITC201611010 | pmid=27802475 }} | |||||||||||||||||||||||||
| Polyarteritis nodosa | Mononeuritis multiplex, nodules, purpura, livedo, and hypertension. | |||||||||||||||||||||||||||||||||||
| Kawasaki disease | last1=Son | first1=M. B. F. | last2=Newburger | first2=J. W. | title=Kawasaki Disease | journal=Pediatrics in Review | volume=34 | issue=4 | date=2013-04-01 | issn=0191-9601 | doi=10.1542/pir.34-4-151 | pages=151–162 | pmid=23547061 }} | |||||||||||||||||||||||
| Microscopic polyangiitis | last1=Chung | first1=Sharon A. | last2=Seo | first2=Philip | title=Microscopic Polyangiitis | journal=Rheumatic Disease Clinics of North America | volume=36 | issue=3 | date=2010 | pmid=20688249 | pmc=2917831 | doi=10.1016/j.rdc.2010.04.003 | pages=545–558}} | |||||||||||||||||||||||
| Granulomatosis with polyangiitis | Crusting rhinorrhea, sinusitis, chronic otitis media, nasal obstruction, shortness of breath, and chronic cough. | |||||||||||||||||||||||||||||||||||
| Eosinophilic granulomatosis with polyangiitis | last1=Vaglio | first1=A. | last2=Buzio | first2=C. | last3=Zwerina | first3=J. | title=Eosinophilic granulomatosis with polyangiitis (Churg–Strauss): state of the art | journal=Allergy | volume=68 | issue=3 | date=2013 | issn=0105-4538 | doi=10.1111/all.12088 | pages=261–273 | pmid=23330816 }} | |||||||||||||||||||||
| Anti-glomerular basement membrane disease | Glomerulonephritis, lung hemorrhage, hematuria, hemoptysis, cough, and dyspnea. | |||||||||||||||||||||||||||||||||||
| Cryoglobulinemic vasculitis | Palpable purpura, Raynaud's phenomenon, joint pain, and peripheral neuropathy. | |||||||||||||||||||||||||||||||||||
| IgA vasculitis | Palpable purpura, arthralgia, abdominal pain, nephritis, and haematuria. | |||||||||||||||||||||||||||||||||||
| Hypocomplementemic urticarial vasculitis | last1=Gu | first1=Stephanie L. | last2=Jorizzo | first2=Joseph L. | title=Urticarial vasculitis | journal=International Journal of Women's Dermatology | volume=7 | issue=3 | date=2021 | pmid=34222586 | pmc=8243153 | doi=10.1016/j.ijwd.2021.01.021 | pages=290–297}} | |||||||||||||||||||||||
| Behçet's disease | Oral ulcers, genital ulcers, papulopustular lesions, uveitis, superficial venous thrombosis and deep vein thrombosis. | |||||||||||||||||||||||||||||||||||
| Cogan syndrome | last1=Iliescu | first1=Daniela Adriana | last2=Timaru | first2=Cristina Mihaela | last3=Batras | first3=Mehdi | last4=Simone | first4=Algerino De | last5=Stefan | first5=Cornel | title=COGAN'S SYNDROME | journal=Romanian Journal of Ophthalmology | publisher=Romanian Society of Ophthalmology | volume=59 | issue=1 | date=2024-03-14 | pages=6–13 | pmid=27373108 | pmc=5729811 }} | |||||||||||||||||
| Cutaneous small-vessel vasculitis | last1=Russell | first1=James P. | last2=Gibson | first2=Lawrence E. | title=Primary cutaneous small vessel vasculitis: approach to diagnosis and treatment | journal=International Journal of Dermatology | volume=45 | issue=1 | date=2006 | issn=0011-9059 | doi=10.1111/j.1365-4632.2005.02898.x | pages=3–13 | pmid=16426368 }} | |||||||||||||||||||||||
| Cutaneous arteritis | last=Furukawa | first=Fukumi | title=Cutaneous Polyarteritis Nodosa: An Update | journal=Annals of Vascular Diseases | publisher=Editorial Committee of Annals of Vascular Diseases | volume=5 | issue=3 | date=2012 | pages=282–288 | pmid=23555526 | doi=10.3400/avd.ra.12.00061 | pmc=3595843 }} | ||||||||||||||||||||||||
| Primary central nervous system vasculitis | last1=Junek | first1=Mats | last2=Perera | first2=Kanjana S | last3=Kiczek | first3=Matthew | last4=Hajj-Ali | first4=Rula A | title=Current and future advances in practice: a practical approach to the diagnosis and management of primary central nervous system vasculitis | journal=Rheumatology Advances in Practice | volume=7 | issue=3 | date=2023-08-26 | article-number=rkad080 | issn=2514-1775 | pmid=38091383 | pmc=10712448 | doi=10.1093/rap/rkad080 }} | ||||||||||||||||||
| Retinal vasculitis | last1=Abu El-Asrar | first1=Ahmed M. | last2=Herbort | first2=Carl P. | last3=Tabbara | first3=Khalid F. | title=Retinal Vasculitis | journal=Ocular Immunology and Inflammation | volume=13 | issue=6 | date=2005 | issn=0927-3948 | doi=10.1080/09273940591003828 | pages=415–433 | pmid=16321886 }} | |||||||||||||||||||||
| Lupus vasculitis | last1=Leone | first1=Patrizia | last2=Prete | first2=Marcella | last3=Malerba | first3=Eleonora | last4=Bray | first4=Antonella | last5=Susca | first5=Nicola | last6=Ingravallo | first6=Giuseppe | last7=Racanelli | first7=Vito | title=Lupus Vasculitis: An Overview | journal=Biomedicines | publisher=MDPI AG | volume=9 | issue=11 | date=2021-11-05 | issn=2227-9059 | doi=10.3390/biomedicines9111626 | doi-access=free | page=1626 | pmid=34829857 | pmc=8615745 | hdl=11572/386878 | hdl-access=free }} | ||||||||
| Rheumatoid vasculitis | last1=Bartels | first1=Christie M. | last2=Bridges | first2=Alan J. | title=Rheumatoid Vasculitis: Vanishing Menace or Target for New Treatments? | journal=Current Rheumatology Reports | publisher=Springer Science and Business Media LLC | volume=12 | issue=6 | date=2010-09-15 | issn=1523-3774 | doi=10.1007/s11926-010-0130-1 | pages=414–419 | pmid=20842467 | pmc=2950222 }} |
Causes
There are several different etiologies for vasculitides. Although infections usually involve vessels as a component of more extensive tissue damage, they can also directly or indirectly cause vasculitic syndromes through immune-mediated secondary events. Simple vascular thrombosis usually only affects the luminal process, but through the process of thrombus organization, it can also occasionally cause a more chronic vasculitic syndrome. The autoimmune etiologies, a particular family of diseases characterized by dysregulated immune responses that produce particular pathophysiologic signs and symptoms, are more prevalent.
Classification
Primary systemic, secondary, and single-organ vasculitides are distinguished using the highest classification level in the 2012 Chapel Hill Consensus Conference nomenclature.
Primary systemic vasculitis
Main article: Systemic vasculitis
Primary systemic vasculitis is categorized by the size of the vessels mainly involved. Primary systemic vasculitis includes large-vessel vasculitis, medium-vessel vasculitides, small-vessel vasculitides, and variable-vessel vasculitides.
Large vessel vasculitis
The 2012 Chapel Hill Consensus Conference defines large vessel vasculitis (LVV) as a type of vasculitis that can affect any size artery. It usually affects the aorta and its major branches more frequently than other vasculitides. Takayasu arteritis (TA) and giant cell arteritis (GCA) are the two main forms of LVV.
Medium vessel vasculitis
Medium vessel vasculitis (MVV) is a type of vasculitis that mostly affects the medium arteries, which are the major arteries that supply the viscera and their branches. Any size artery could be impacted, though. The two primary types are polyarteritis nodosa (PAN) and Kawasaki disease (KD).
Small vessel vasculitis
Small vessel vasculitis (SVV) is separated into immune complex SVV and antineutrophil cytoplasmic antibody (ANCA)-associated vasculitis (AAV).
Antineutrophil cytoplasmic antibody (ANCA)-associated vasculitis (AAV) is a necrotizing vasculitis linked to MPO-ANCA or PR3-ANCA that primarily affects small vessels and has few or no immune deposits. AAV is further classified as eosinophilic granulomatosis with polyangiitis (EGPA), granulomatosis with polyangiitis (GPA), and microscopic polyangiitis (MPA).
Immune complex small vessel vasculitis (SVV) is a vasculitis that primarily affects small vessels and has moderate to significant immunoglobulin and complement component deposits on the vessel wall. Normocomplementemic urticarial vasculitis (HUV) (anti-C1q vasculitis), cryoglobulinemic vasculitis (CV), IgA vasculitis (Henoch–Schönlein) (IgAV), and anti-glomerular basement membrane (anti-GBM) disease are the categories of immune complex SVV.
Variable vessel vasculitis
Variable vessel vasculitis (VVV) is a kind of vasculitis that may impact vessels of all sizes (small, medium, and large) and any type (arteries, veins, and capillaries), with no particular type of vessel being predominantly affected. This category includes Behcet's disease (BD) and Cogan's syndrome (CS).
Secondary vasculitis
The subset of illnesses known as secondary vasculitides is believed to be triggered by an underlying ailment or exposure. Systemic illnesses (such as rheumatoid arthritis), cancer, drug exposure, and infection are the primary causes of vasculitis; however, there are still a few factors that have a conclusively shown pathogenic relationship to the condition. Vasculitis frequently coexists with infections, and several infections, including hepatitis B and C, HIV, infective endocarditis, and tuberculosis, are significant secondary causes of vasculitis. Except for rheumatoid vasculitis, the majority of secondary vasculitis forms are exceedingly rare.
Single-organ vasculitis
Single-organ vasculitis, formerly known as "localized", "limited", "isolated", or "nonsystemic" vasculitis, refers to vasculitis that is limited to one organ or organ system. Examples of this type of vasculitis include gastrointestinal, cutaneous, and peripheral nerve vasculitides.
Diagnosis
- Laboratory tests of blood or body fluids are performed for patients with active vasculitis. Their results will generally show signs of inflammation in the body, such as increased erythrocyte sedimentation rate (ESR), elevated C-reactive protein (CRP), anemia, increased white blood cell count and eosinophilia. Other possible findings are elevated antineutrophil cytoplasmic antibody (ANCA) levels and hematuria.
- Other organ functional tests may be abnormal. Specific abnormalities depend on the degree of organ involvement. A brain SPECT can show decreased blood flow to the brain and brain damage.
- The definite diagnosis of vasculitis is established after a biopsy of involved organ or tissue, such as skin, sinuses, lung, nerve, brain, and kidney. The biopsy elucidates the pattern of blood vessel inflammation. :*Some types of vasculitides display leukocytoclasis, which is vascular damage caused by nuclear debris from infiltrating neutrophils. It typically presents as palpable purpura. Conditions with leucocytoclasis mainly include hypersensitivity vasculitis (also called leukocytoclastic vasculitis) and cutaneous small-vessel vasculitis (also called cutaneous leukocytoclastic angiitis).
- An alternative to biopsy can be an angiogram (x-ray test of the blood vessels). It can demonstrate characteristic patterns of inflammation in affected blood vessels.
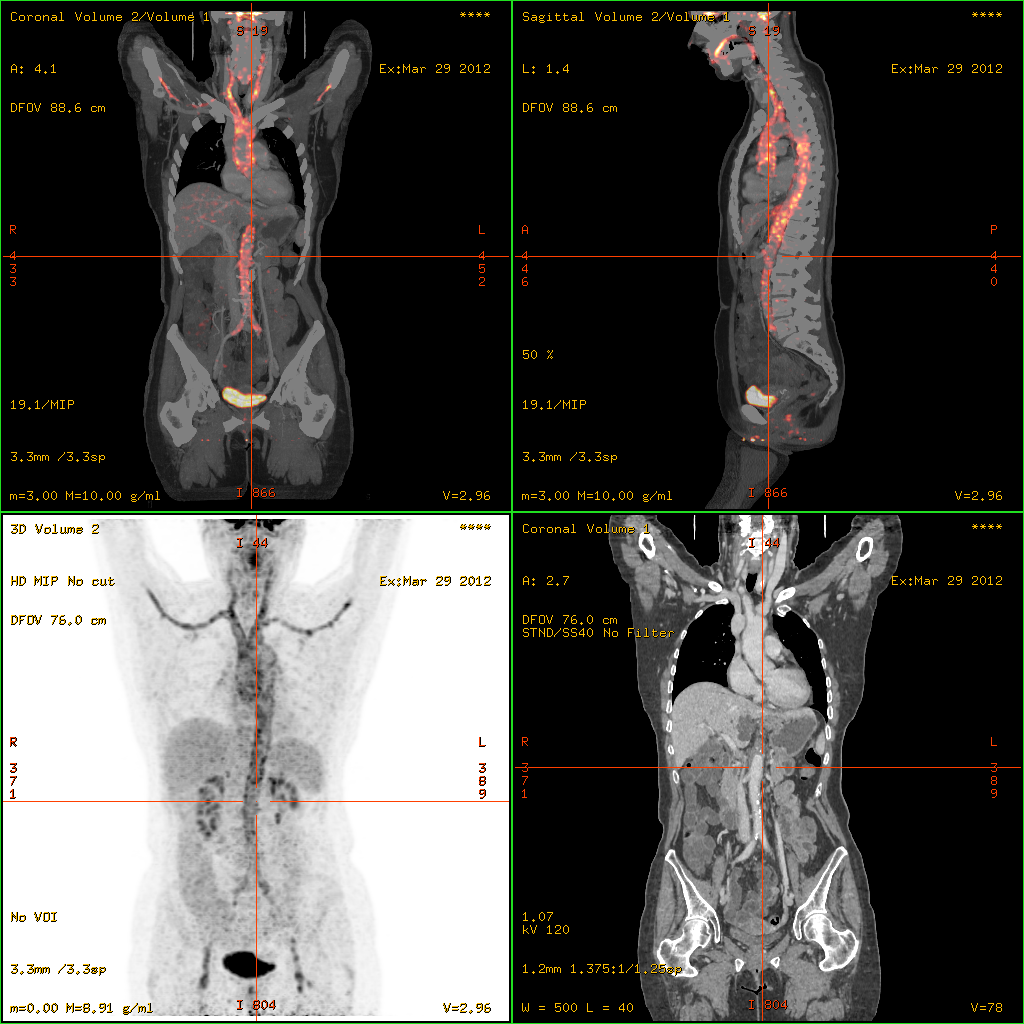
- 18F-fluorodeoxyglucose positron emission tomography/computed tomography (FDG-PET/CT)has become a widely used imaging tool in patients with suspected Large Vessel Vasculitis, due to the enhanced glucose metabolism of inflamed vessel walls. The combined evaluation of the intensity and the extension of FDG vessel uptake at diagnosis can predict the clinical course of the disease, separating patients with favourable or complicated progress.
- Acute onset of vasculitis-like symptoms in small children or babies may instead be the life-threatening purpura fulminans, usually associated with severe infection.
| Disease | Serologic test | Antigen | Associated laboratory features |
|---|---|---|---|
| Systemic lupus erythematosus | ANA including antibodies to dsDNA and ENA [including SM, Ro (SSA), La (SSB), and RNP] | Nuclear antigens | Leukopenia, thrombocytopenia, Coombs' test, complement activation: low serum concentrations of C3 and C4, positive immunofluorescence using Crithidia luciliae as substrate, antiphospholipid antibodies (i.e. anticardiolipin, lupus anticoagulant, false-positive VDRL) |
| Goodpasture's disease | Anti-glomerular basement membrane antibody | Epitope on noncollagen domain of type IV collagen | |
| Small vessel vasculitis | |||
| Microscopic polyangiitis | Perinuclear antineutrophil cytoplasmic antibody | Myeloperoxidase | Elevated CRP |
| Granulomatosis with polyangiitis | Cytoplasmic antineutrophil cytoplasmic antibody | Proteinase 3 (PR3) | Elevated CRP |
| Eosinophilic granulomatosis with polyangiitis | perinuclear antineutrophil cytoplasmic antibody in some cases | Myeloperoxidase | Elevated CRP and eosinophilia |
| IgA vasculitis (Henoch–Schönlein purpura) | None | ||
| Cryoglobulinemia | Cryoglobulins, rheumatoid factor, complement components, hepatitis C | ||
| Medium vessel vasculitis | |||
| Classical polyarteritis nodosa | None | Elevated CRP and eosinophilia | |
| Kawasaki's Disease | None | Elevated CRP and ESR |
In this table: ANA = antinuclear antibodies, CRP = C-reactive protein, ESR = erythrocyte sedimentation rate, dsDNA = double-stranded DNA, ENA = extractable nuclear antigens, RNP = ribonucleoproteins; VDRL = Venereal Disease Research Laboratory
Treatment
Treatments are generally directed toward stopping the inflammation and suppressing the immune system. Typically, corticosteroids such as prednisone are used. Additionally, other immune suppression medications, such as cyclophosphamide, are considered. In case of an infection, antimicrobial agents including cephalexin may be prescribed. Affected organs (such as the heart or lungs) may require specific medical treatment intended to improve their function during the active phase of the disease.
References
References
- "Vasculitis — Definition".
- "Glossary of dermatopathological terms. DermNet NZ".
- {{DorlandsDict. eight/000114505. Vasculitis
- Sunderkötter, Cord. (2022). "Braun-Falco´s Dermatology". Springer Berlin Heidelberg.
- (August 2018). "Diagnosis and Treatment in Internal Medicine". Oxford University Press.
- Jayne, David. (2009). "The diagnosis of vasculitis". Best Practice & Research Clinical Rheumatology.
- (2018). "Vasculitis—What Do We Have to Know? A Review of Literature". The International Journal of Lower Extremity Wounds.
- (2024-03-14). "Takayasu arteritis: a review". BMJ Publishing Group.
- Hoffman, Gary S.. (2016-11-01). "Giant Cell Arteritis". Annals of Internal Medicine.
- (2015). "Polyarteritis Nodosa". Rheumatic Disease Clinics of North America.
- (2013-04-01). "Kawasaki Disease". Pediatrics in Review.
- (2018-07-10). "Kawasaki Disease". Frontiers in Pediatrics.
- (2010). "Microscopic Polyangiitis". Rheumatic Disease Clinics of North America.
- (16 October 2025). "Challenges in the diagnosis, classification and prognosis of ANCA-associated vasculitis.". Nat Rev Rheumatol.
- (2014). "Granulomatosis with polyangiitis (Wegener): Clinical aspects and treatment". Autoimmunity Reviews.
- (2018-10-03). "Clinical manifestations of granulomatosis with polyangiitis: key considerations and major features". Postgraduate Medicine.
- (16 October 2025). "Challenges in the diagnosis, classification and prognosis of ANCA-associated vasculitis.". Nat Rev Rheumatol.
- (2013). "Eosinophilic granulomatosis with polyangiitis (Churg–Strauss): state of the art". Allergy.
- (2023). "Eosinophilic granulomatosis with polyangiitis: A review". Autoimmunity Reviews.
- (16 October 2025). "Challenges in the diagnosis, classification and prognosis of ANCA-associated vasculitis.". Nat Rev Rheumatol.
- (2024). "Anti–Glomerular Basement Membrane Disease: Recent Updates". Advances in Kidney Disease and Health.
- (2019). "New insights in cryoglobulinemic vasculitis". Journal of Autoimmunity.
- (2021). "IgA vasculitis". Seminars in Immunopathology.
- (2021). "Urticarial vasculitis". International Journal of Women's Dermatology.
- (2020-05-01). "Behçet: the syndrome". Rheumatology.
- (2024-03-14). "COGAN'S SYNDROME". Romanian Society of Ophthalmology.
- (2021). "Localized Forms of Vasculitis". Current Rheumatology Reports.
- (2006). "Primary cutaneous small vessel vasculitis: approach to diagnosis and treatment". International Journal of Dermatology.
- Furukawa, Fukumi. (2012). "Cutaneous Polyarteritis Nodosa: An Update". Editorial Committee of Annals of Vascular Diseases.
- (2023-08-26). "Current and future advances in practice: a practical approach to the diagnosis and management of primary central nervous system vasculitis". Rheumatology Advances in Practice.
- (2005). "Retinal Vasculitis". Ocular Immunology and Inflammation.
- (2021-11-05). "Lupus Vasculitis: An Overview". MDPI AG.
- (2010-09-15). "Rheumatoid Vasculitis: Vanishing Menace or Target for New Treatments?". Springer Science and Business Media LLC.
- Seidman, M.A.. (2014). "Pathobiology of Human Disease". Elsevier.
- (27 December 2012). "2012 Revised International Chapel Hill Consensus Conference Nomenclature of Vasculitides". Wiley.
- Jennette, J. Charles. (27 September 2013). "Overview of the 2012 revised International Chapel Hill Consensus Conference nomenclature of vasculitides". Springer Science and Business Media LLC.
- (2015). "Classification and classification criteria for vasculitis". Ovid Technologies (Wolters Kluwer Health).
- Suresh, E. (1 August 2006). "Diagnostic approach to patients with suspected vasculitis". Oxford University Press (OUP).
- (2005). "How to diagnose and treat secondary forms of vasculitis". Elsevier BV.
- Eastham, A Brooke W. (12 July 2021). "Leukocytoclastic Vasculitis: Practice Essentials, Pathophysiology, Etiology".
- (2014-10-23). "Giant-Cell Arteritis and Polymyalgia Rheumatica". New England Journal of Medicine.
- (2016). "The prognostic value of baseline 18F-FDG PET/CT in steroid-naïve large-vessel vasculitis: introduction of volume-based parameters". European Journal of Nuclear Medicine and Molecular Imaging.
- (2012). "Tietz Textbook of Clinical Chemistry and Molecular Diagnostics". Saunders.
This article was imported from Wikipedia and is available under the Creative Commons Attribution-ShareAlike 4.0 License. Content has been adapted to SurfDoc format. Original contributors can be found on the article history page.
Ask Mako anything about Vasculitis — get instant answers, deeper analysis, and related topics.
Research with MakoFree with your Surf account
Create a free account to save articles, ask Mako questions, and organize your research.
Sign up freeThis content may have been generated or modified by AI. CloudSurf Software LLC is not responsible for the accuracy, completeness, or reliability of AI-generated content. Always verify important information from primary sources.
Report