From Surf Wiki (app.surf) — the open knowledge base
Focal segmental glomerulosclerosis
Kidney disease
Kidney disease
| Field | Value |
|---|---|
| name | Focal segmental glomerulosclerosis |
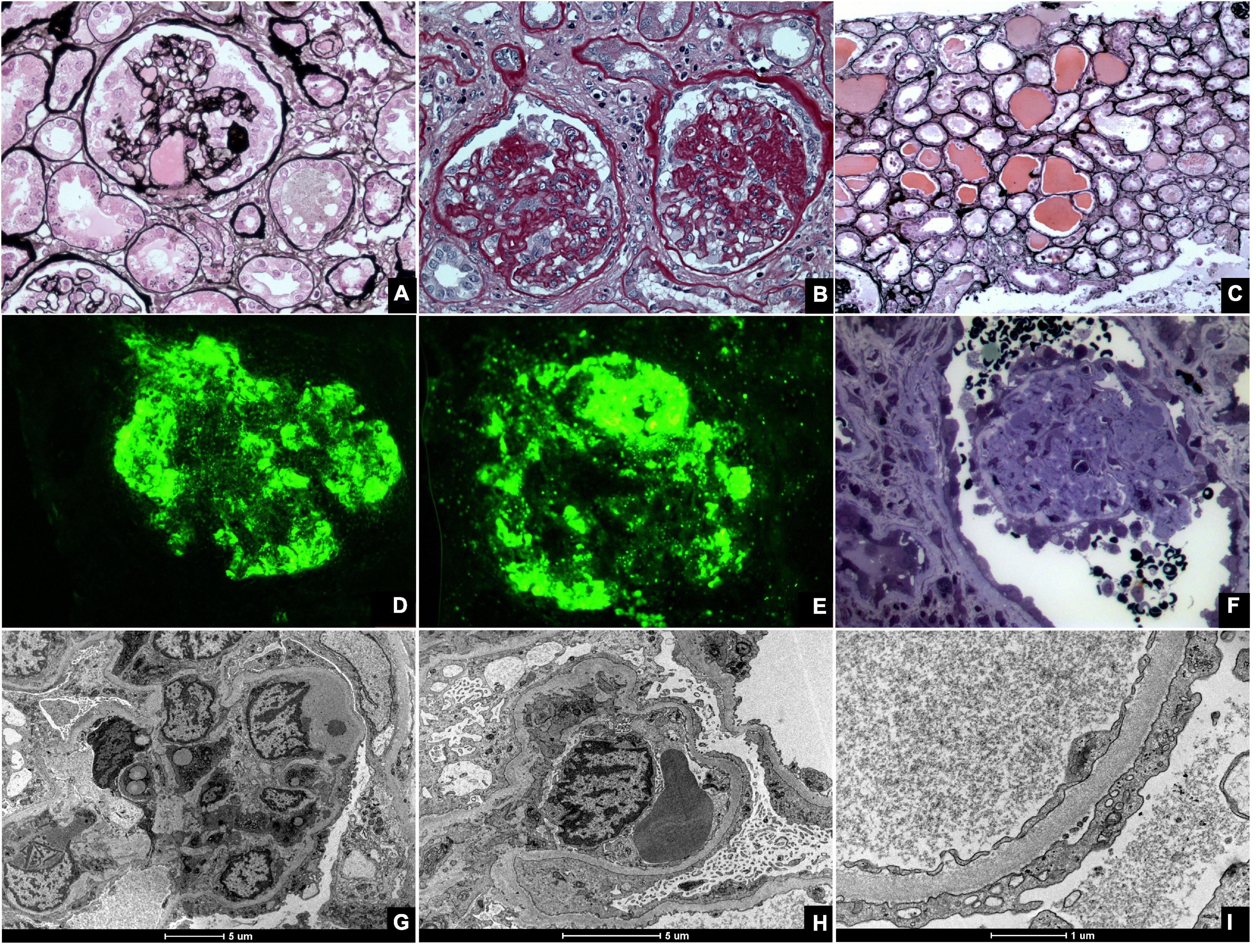
| image | Focal segmental glomerulosclerosis - high mag.jpg |
| caption | Light micrograph of focal segmental glomerulosclerosis, hilar variant. Kidney biopsy. PAS stain. |
| synonyms | focal glomerular sclerosis, focal nodular glomerulosclerosis |
| Focal segmental glomerulosclerosis (FSGS) is a histopathologic finding of scarring (sclerosis) of glomeruli and damage to renal podocytes. This process damages the filtration function of the kidney, resulting in protein presence in the urine due to protein loss. FSGS is a leading cause of excess protein loss—nephrotic syndrome—in children and adults in the US. Signs and symptoms include proteinuria and edema. Kidney failure is a common long-term complication of the disease. FSGS can be classified as primary, secondary, or genetic, depending on whether a particular toxic or pathologic stressor or genetic predisposition can be identified as the cause. and treatment consists of glucocorticoids and other immune-modulatory drugs. Response to therapy is variable, with a significant portion of patients progressing to end-stage kidney failure.
Signs and symptoms
The most common symptoms are a result of abnormal loss of protein from the glomerulus of the kidney, and include:
- Frothy urine (due to excess protein)
- Excess water retention (pitting edema, due to loss of serum albumin)
- Susceptibility to infection (due to loss of serum antibodies)
Common signs are also due to loss of blood proteins by the glomerulus of the kidney, including:
- Protein in the urine (often in the nephrotic syndrome-range of 3.5 g/day)
- Low serum albumin (
- Low serum antibodies
- High serum cholesterol (compensatory by the liver to compensate for low serum oncotic pressure)
- Fatty casts in the urine (secondary to hypercholesterolemia)
Pathophysiology
FSGS is primarily a disease of the renal glomerulus, the site of filtration of ions and solutes. Podocytes are specialized cells lining the Bowman's capsule that contribute to the filtration barrier, preventing molecules larger than 5 nm from being filtered. FSGS involves damage to the renal podocytes such that larger molecules, most notably proteins, are filtered and lost through the kidney. Thus, many of the signs and symptoms of FSGS are related to protein loss.
On histology, FSGS manifests as scarring (sclerosis) to segments of glomeruli; moreover, only a portion of glomeruli are affected. The focal and segmental nature of disease seen on histology help to distinguish FSGS from other types of glomerular sclerosis.
FSGS can be classified by the putative cause of damage to podocytes. Primary FSGS involves cases in which no cause is readily identifiable. It is presumed that a set of unidentified circulating factors in the blood contribute to podocyte damage in these cases.
Secondary FSGS is caused by an identifiable stress or toxin that injures podocytes. Hyperfiltration can be caused by obesity, diabetes or loss of the contralateral kidney, among other causes.
Secondary FSGS can also be caused by toxins, including anabolic steroids and heroin.
A number of genes have been implicated in FSGS. These include: NPHS1, which encodes the protein nephrin that contributes to the filtration barrier; NPHS2, which encodes the protein podocin found in podocytes; and INF2, which encodes the actin-binding protein formin.
The pathogenesis of HIV-associated FSGS is unclear, but may be due to the presence of the G1/G2 risk alleles of the APOL1 gene. There is some data to suggest that HIV can infect tubular epithelial cells and podocytes, but much remains to be known.
Gain of function mutations in APOL1 have also been proposed to play a role in the pathogenesis of this disease.
Diagnosis
Diagnosis of FSGS is made by renal biopsy that includes at least fifteen serial cuts with at least eight glomeruli. Histologic features include sclerosis (scarring) of a portion (average: 15%) of the glomerular space, with only a portion of glomeruli manifesting any sclerosis.
Other tests helpful in the diagnosis include urine protein, urinalysis, serum albumin, and serum lipids. A clinical picture of proteinuria, low blood protein levels (albumin, antibodies), and high blood cholesterol would support a diagnosis of FSGS, although these do not help to distinguish between FSGS and other causes of proteinuria.
Classification
Five mutually exclusive variants of focal segmental glomerulosclerosis may be distinguished by the pathologic findings seen on renal biopsy:
- Collapsing variant
- Glomerular tip lesion variant
- Cellular variant
- Perihilar variant
- Not otherwise specified (NOS) variant
Recognition of these variants may have prognostic value in individuals with primary focal segmental glomerulosclerosis. The collapsing variant is associated with higher rate of progression to end-stage renal disease, whereas the glomerular tip lesion variant has a low rate of progression to end-stage renal disease in most patients. The cellular variant shows similar clinical presentation to collapsing and glomerular tip variant but has intermediate outcomes between the other two variants.
Treatment
First-line treatment for primary FSGS consists of anti-inflammatory drugs. For patients who maintain nephrotic-range proteinuria despite glucocorticoids, or for patients who demonstrate glucocorticoid intolerance, calcineurin inhibitors (e.g., tacrolimus) are initiated. Successful treatment is defined as a drop in proteinuria to sub-nephrotic ranges.
The treatment of secondary FSGS involves addressing the particular toxic or stress agent.
Prognosis
The majority of untreated cases of FSGS will progress to end-stage kidney disease. Important prognostic factors include the degree of proteinuria and initial response to therapy.
Patients with nephrotic-range (3.5 g/day) proteinuria have over a 50% rate of progression to end-stage kidney disease at 10 years. Only 15% of patients with sub-nephrotic ranges of proteinuria progress to end-stage renal failure at 10 years.
Initial response to therapy also dictates long-term outcomes. Those defined as having a "complete response" typically manifest a proteinuria of
Epidemiology
FSGS accounts for 35% of all cases of nephrotic syndrome, making it one of the most common causes of nephrotic syndrome in the United States. FSGS accounts for 2% of all cases of kidney failure. African American patients have four times the likelihood of developing FSGS. Men are about two times as likely to develop FSGS compared to women.
Notable cases
- Andy Cole
- Gary Coleman
- Sean Elliott
- Alonzo Mourning
References
References
- "focal segmental glomerulosclerosis" at ''[[Dorland's medical reference works. Dorland's Medical Dictionary]].''
- (March 2017). "Focal Segmental Glomerulosclerosis". Clin J Am Soc Nephrol.
- (November 2004). "Twenty-one-year trend in ESRD due to focal segmental glomerulosclerosis in the United States". Am J Kidney Dis.
- (April 1995). "Focal segmental glomerular sclerosis in adults: presentation, course, and response to treatment". Am J Kidney Dis.
- (June 1994). "Primary focal segmental glomerulosclerosis: clinical course and response to therapy". Am J Kidney Dis.
- (2021-10-28). "Focal segmental glomerulosclerosis (FSGS)".
- (November 1997). "Changing etiologies of unexplained adult nephrotic syndrome: a comparison of renal biopsy findings from 1976–1979 and 1995–1997". Am J Kidney Dis.
- (September 2011). "Focal segmental glomerulosclerosis and chronic kidney disease in pediatric patients". Adv Chronic Kidney Dis.
- (2018). "Protecting Podocytes: A Key Target for Therapy of Focal Segmental Glomerulosclerosis". Am J Nephrol.
- (March 2003). "Trends in the epidemiology of focal segmental glomerulosclerosis". Semin Nephrol.
- (November 1998). "Anatomy and physiology of the kidney". AORN J.
- (August 2014). "The glomerulus: the sphere of influence". Clin J Am Soc Nephrol.
- (2012). "Mechanisms of glomerular albumin filtration and tubular reabsorption". Int J Nephrol.
- (June 2016). "Podocyte injury and its consequences". Kidney Int.
- (February 2019). "Nephrotic Syndrome". Pediatr Clin North Am.
- "Focal Segmental Glomerulosclerosis (FSGS)".
- (June 1996). "Focal segmental glomerulosclerosis". Pediatr Nephrol.
- (August 2017). "Focal segmental glomerulosclerosis; why does it occur segmentally?". Pflugers Arch.
- (March 2018). "Differentiating Primary, Genetic, and Secondary FSGS in Adults: A Clinicopathologic Approach". J Am Soc Nephrol.
- (June 1989). "Pathogenesis and significance of nonprimary focal and segmental glomerulosclerosis". Am J Kidney Dis.
- (January 1985). "The changing spectrum of heroin-associated nephropathy". Am J Kidney Dis.
- (June 1986). "Renal disease in patients with massive obesity". Arch Intern Med.
- (October 2008). "Nephrin mutations can cause childhood-onset steroid-resistant nephrotic syndrome". J Am Soc Nephrol.
- (April 2000). "NPHS2, encoding the glomerular protein podocin, is mutated in autosomal recessive steroid-resistant nephrotic syndrome". Nat Genet.
- (January 2010). "Mutations in the formin gene INF2 cause focal segmental glomerulosclerosis". Nat Genet.
- Chang, Anthony, Robbins & Cotran Pathologic Basis of Disease, Chapter 20, 895–952
- (November 2011). "APOL1 genetic variants in focal segmental glomerulosclerosis and HIV-associated nephropathy". J Am Soc Nephrol.
- (January 1996). "Serial morphometric analysis of sclerotic lesions in primary "focal" segmental glomerulosclerosis". J Am Soc Nephrol.
- (December 1993). "Primary focal segmental glomerulosclerosis: pathology, histological variants, and pathogenesis". Am J Kidney Dis.
- (2022). "Collapsing Glomerulopathy: A Review by the Collapsing Brazilian Consortium.". Front Med (Lausanne).
- (March 2006). "Clinical and pathologic characteristics of focal segmental glomerulosclerosis pathologic variants". Kidney Int.
- Fogo AB. (February 2015). "Causes and pathogenesis of focal segmental glomerulosclerosis". Nat Rev Nephrol.
- (July 2015). "Focal segmental glomerulosclerosis: molecular genetics and targeted therapies". BMC Nephrol.
- (2020). "Extracorporeal Therapies in the Treatment of Focal Segmental Glomerulosclerosis". Blood Purif.
- (November 2005). "Idiopathic focal segmental glomerulosclerosis: a favourable prognosis in untreated patients?". Neth J Med.
- (April 2005). "Focal and segmental glomerulosclerosis: definition and relevance of a partial remission". J Am Soc Nephrol.
This article was imported from Wikipedia and is available under the Creative Commons Attribution-ShareAlike 4.0 License. Content has been adapted to SurfDoc format. Original contributors can be found on the article history page.
Ask Mako anything about Focal segmental glomerulosclerosis — get instant answers, deeper analysis, and related topics.
Research with MakoFree with your Surf account
Create a free account to save articles, ask Mako questions, and organize your research.
Sign up freeThis content may have been generated or modified by AI. CloudSurf Software LLC is not responsible for the accuracy, completeness, or reliability of AI-generated content. Always verify important information from primary sources.
Report